Anterior Vertebral Body Tethering (AVBT)
Make an Appointment
Our team is here to help you make an appointment with the specialists that you need.
The traditional surgery for scoliosis is called a posterior spinal fusion and instrumentation – or PSIF. This procedure uses a spinal rod placed in the back part of the spine. In July 2019, the FDA approved the use of a newly designed vertebral tether to treat growing children with progressive scoliosis. Similar devices had been previously used in a small group of children over the last 8-10 years, and we have learned a lot from that early experience. Instead of the rod, the tether uses a flexible cord which is placed from the front part of the spine only on the convexity of the curve. This allows correction of the scoliosis but also continued growth on the oppositie (concave), untethered side.
Who is a tether candidate?
The tether is an alternative to spinal fusion for patients with idiopathic scoliosis. Patients who are candidates have:
- A main thoracic curve between 45 and 60 degrees (this is the main curve that gets the tether attached).
- Ideally, the compensatory lumbar curve is smaller than 45 degrees.
- These patients also have a significant amount of bone growth remaining. A hand bone age can be used to determine the bone growth but most candidates are 8-13 years of age.
Preparing for surgery:
The preparation of the surgery is similar to the traditional procedure. The tether is a braided cord that is attached to the spine at the apex of the curve during a surgical procedure in the operating room. Pre-operative planning includes some special tests and appointments:
- A spine screening MRI to look at soft tissues around your spine
- A Pulmonary Function Test (PFTs) to evaluate lung function
- Bending X-Rays to evaluate the flexibility of the curve
- Blood work that needs to be done at the Children’s Hospital
- Pediatrician pre-op appointment for clearance
- Pre-op appointment with your surgeon to address any additional questions
- Typically post-procedure patients are admitted to the hospital for about 3 days.
- A chest tube is placed near the incision during the surgery and will stay for 2-3 days after surgery.
- The bandage is removed in the doctor’s office by a nurse practitioner or physician assistant 10-14 days after the surgery.
Follow up after the tether procedure:
- The tether provides some correction of the main curve immediately after the implantation, however, this is important to monitor throughout growth.
- After surgery there is no casting or bracing.
- The majority of children return to school within 4 weeks and can often return to full activity including sports within 6 months, if not sooner.
- Patients are followed by their surgeon with regular 6 month clinical exam and x-rays until they are skeletally mature.
Success of the procedure:

There have been no studies of the new device, released after the FDA approval in August 2019. However, there have been 5 published and more than 10 as yet unpublished studies of patients who underwent this procedure with the original device before FDA approval. Most people expect that modern day results with the new device and a better understanding of how and when to use the tether will be better than the original results.
Nevertheless, the results of patients undergoing tethering with the original device were overall quite positive. Risks were overall low, and correction of the main curve was very good at about 50-65%. Still traditional surgery consisting of a posterior fusion still probably allows a more complete three dimensional correction of the curve. While there has been some concern about whether the tether might not allow as good correction of shoulder balance compared with the traditional fusion, we did not see that in a study we did of tether, which looked at 81 patients.
However early results of the tether showed that 10-20% of patients undergoing spinal tether needed another operation. This is high when you consider that this rate is probably 1-2% for patients undergoing the traditional fusion surgery. The reason for a second operation included both “overcorrection” (the tether worked too well and created a curve in the opposite direction and also progression of the curve despite tethering which required a fusion in some children. We think that both of these will be less likely now that we understand more about the best age to intervene.
The decision about whether to proceed with tethering or another procedure depends on a number of factors including growth remaining, details of the spinal curvature and your preferences about the tradeoffs involved between avoiding spinal fusion and what is probably a higher chance of needed a second unplanned surgery after tethering.
Risks of the Procedure
Studies have shown that the tether procedure, when performed at a Children’s specialized hospital, had low risk of complications other than the possibility of a second surgery as noted above.
Research Articles:
- Anterior Vertebral Body Tethering for Idiopathic Scoliosis
- Growth Modulation for Childhood Scoliosis: From Where Have We Come, and Where are We Going?
- Growth Modulation by Means of Anterior Tethering
- Multilevel Spinal Growth Modulation With an Anterolateral Flexible Tether in an Immature Bovine Model
- Spinal Growth Modulation With an Anterolateral Flexible Tether in an Immature Bovine Model
Resources
- The Tether Patient Brochure
- Vertebral Body Tethering VBT in Pediatric and Adult Spinal Deformity Scoliosis Research Society
And the comparison of a fusion to a tether:
What is the advantage of Vertebral Tethering?
Vertebral tethering allows for the correction of the scoliosis without fusion of the vertebra in the spine. This allows for continued growth and flexibility at the spine.
How do I know if Vertebral Tethering is right for my child?
Vertebral tethering is an option to correct moderate size spinal curvature (45 – 60 degrees) in a skeletally immature patient (Sanders < 5 on hand x-ray).
What does the surgery involve?
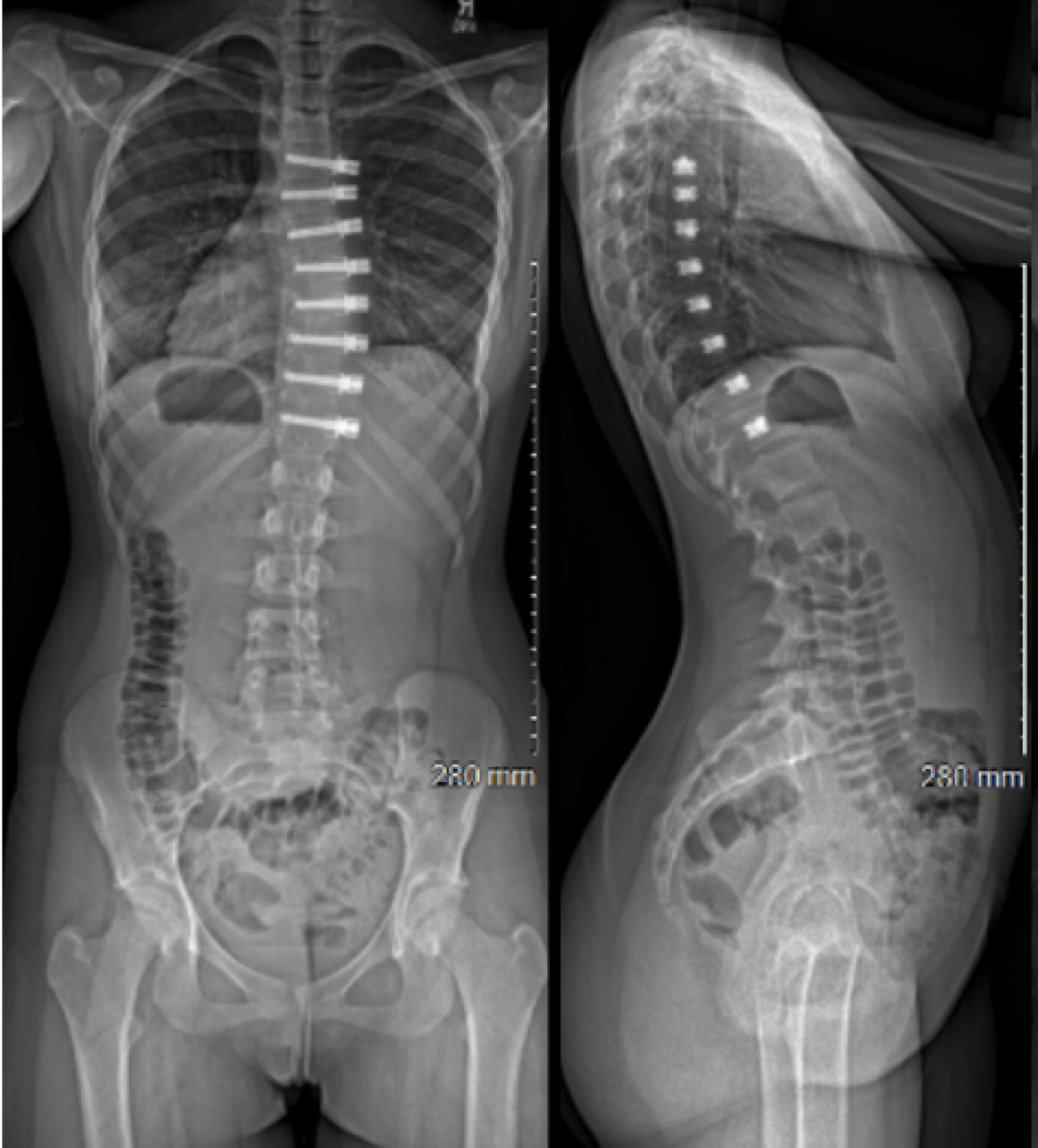
The surgery involves the placement of screws using a thoracoscopic approach. This means that the screws are placed using small ports and a camera in the front/side of the chest. The flexible tether is then attached to those screws.
What are some complications?
Complications of the Vertebral Tethering include: over correction of the main thoracic curve, failure of hardware including tether breakage or screw migration, post-operative pneumothorax, surgical site infection, pleural effusion, right shoulder or arm numbness, and back pain.